Adenoidectomy
Adenoid is a single mass of lymphoid tissue with its base on the posterior nasopharyngeal wall and its apex pointed toward the nasal septum. The surface is invaginated in a series of folds. It is covered by pseudostratified ciliated epithelium and is infiltrated by the lymphoid follicles.
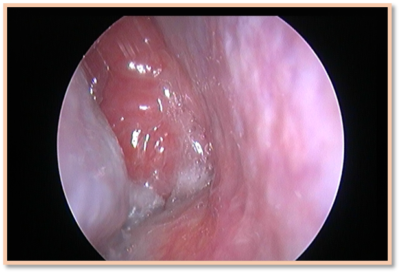
Figure 1 Endoscopic view of enlarged adenoid mass completely filling up and blocking the right choana.
Indications for adenoidectomy:
- A child below 12 years of age presenting with four or more episodes of purulent rhinorrhea in preceding one year.
- A child with persisting symptoms of adenoiditis (purulent nasal discharge, nasal obstruction, and mouth breathing) after two to three weeks of appropriate antibiotic therapy.
- A child with persistent sleep disturbances associated with nasal airway obstruction
- A child with hypo nasal or nasal speech
- A child with otitis media with effusion persisting for three months or longer
- A child with documented dental malocclusion or disturbed Oro-facial growth.

Figure 2 X-ray soft-tissue nasopharynx (lateral view) showing enlarged adenoid mass (shaded red) which is almost completely obstructing the nasopharyngeal airway. Also make note of high arched palate and dental malocclusion secondary to mouth breathing.
Contraindications of adenoidectomy include a sub-mucosal cleft palate that may result in post-op velopharyngeal insufficiency. If there is a strong case for adenoidectomy in such a patient only upper half of adenoid tissue is removed. In such a situation lower half act as a cushion for soft palate and helps in closure of velo-pharyngeal isthmus. Adenoidectomy is delayed by six-weeks in a child who has recently received a dose of oral polio vaccination.
Adenoidectomy is always performed under general anesthesia with airway properly secured. Patient is placed in supine position. Neck of the patient is extended by placing a sandbag under the shoulders (over extension of the neck is avoided). Head of the patient is stabilised by placing a ring below it. Headend of the operation table is lowered.
The surgeon first visualises the adenoid mass by lifting the soft palate for its appearance and any abnormal pulsations. Then mass is palpated for any abnormal pulsations. In case there is any abnormal pulsation the procedure is abandoned.
Then the adenoid curette with guard is engaged in adenoid tissue and curette is moved downwards with a sustained movement (with fulcrum of the movement at wrist joint) without using any undue force. The adenoid issue gets sliced and is removed. Nasopharynx is packed with ribbon gauze and pressure is applied to control the bleeding.
After the bleeding has been controlled, pack is removed, and nasopharynx inspected for any left-over tissue tags. The tags are plucked with the help of a Luc’s forceps. Nasopharynx is packed again with ribbon gauze and pressure applied till bleeding stops.
Once the bleeding has been controlled, throat packs are removed, and patient shifted after patient is given green signal by anesthetist.
The common complications of the procedure include:
- Haemorrhage, both primary and secondary
- Vomiting
- Dehydration
- Airway obstruction due to edema
- Pulmonary edema
- Fever, velopharyngeal insufficiency
- Dental injury
- Burns
- Nasopharyngeal stenosis
Atlantoaxial subluxation can occur in patients with Down syndrome. Atlantoaxial joint laxity may occur because of Grisel’s syndrome. This is vertebral body decalcification and laxity of the anterior transverse ligament between the atlas and the axis from inflammation or infection in the nasopharynx. Spontaneous subluxation occurs about one week post operatively with pain and torticollis.
Buy Paperback or Kindle edition
Amazon US:
https://www.amazon.com/dp/B08NSCTK11Amazon Canada:
https://www.amazon.ca/dp/B08NSCTK11Amazon UK:
https://www.amazon.co.uk/dp/B08NSCTK11Amazon Australia:
https://www.amazon.com.au/dp/B08NSCTK11Amazon India:
https://www.amazon.in/dp/B08NY42JD6